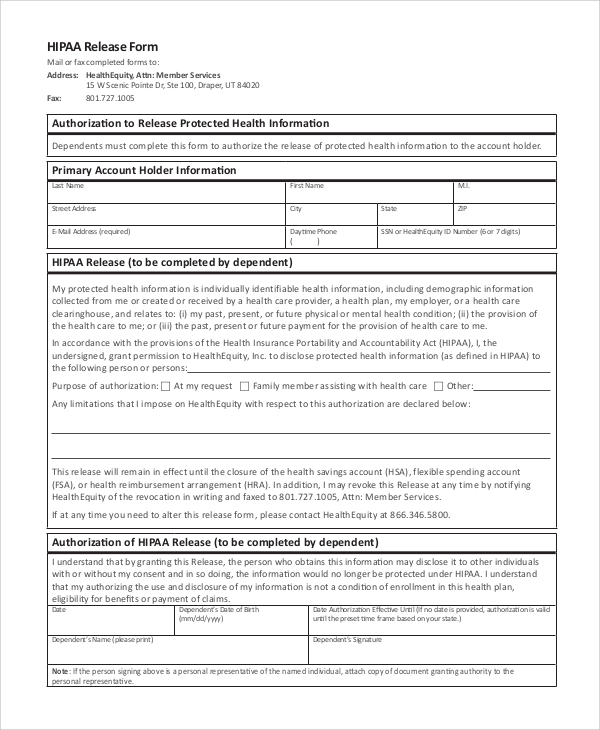
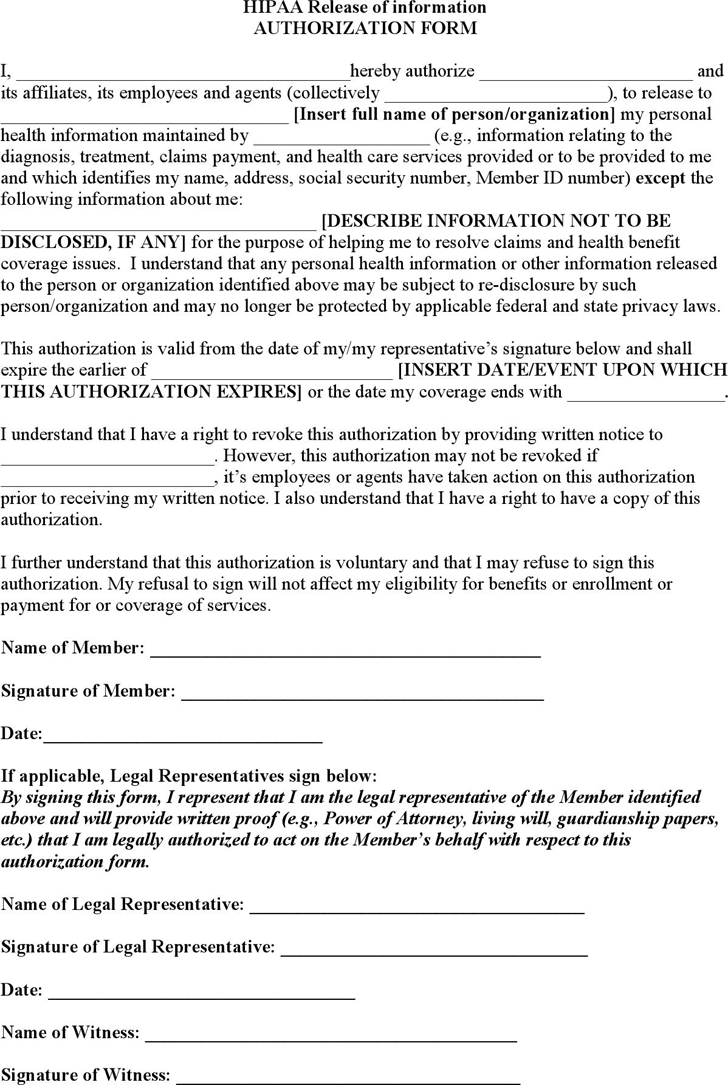
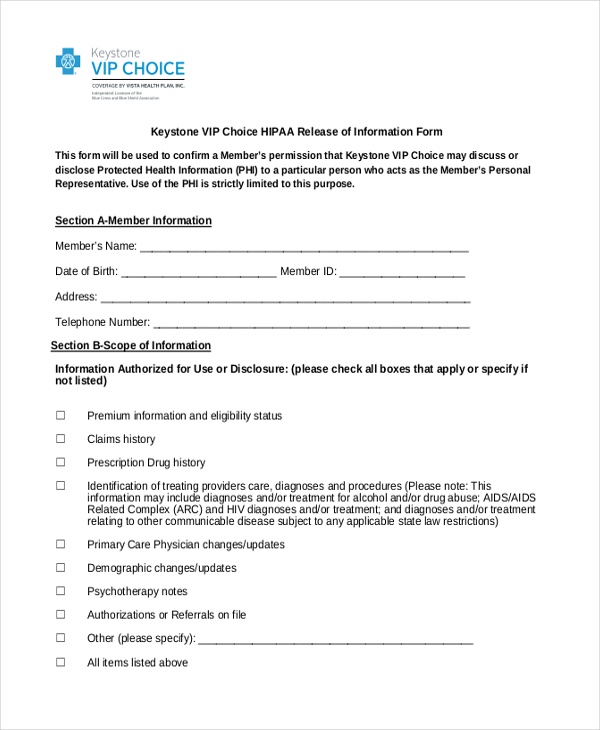
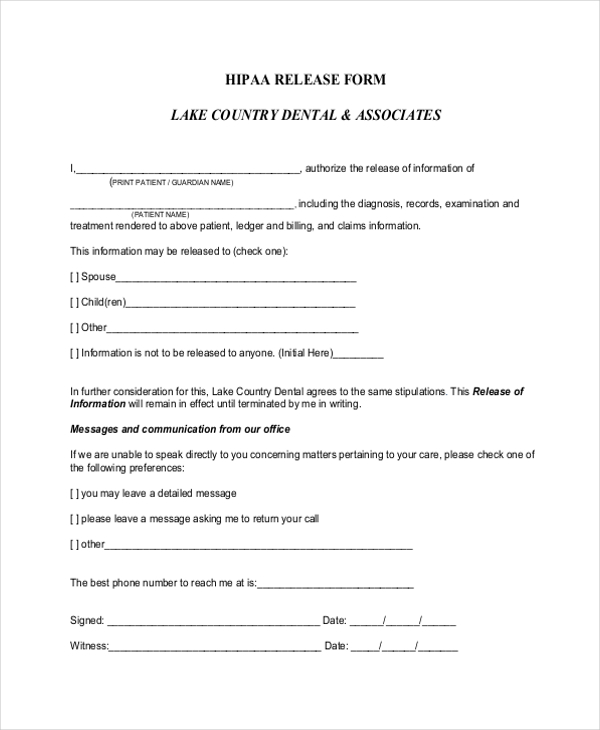
Hipaa Release Of Information Form Template. Extent of Authorization** a. □ I authorize the release of my complete health record (including records relating to mental healthcare, communicable. I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form HIPAA Release Form.

This authorized form is used to release a particular patient's health information.
Authorization for the Release of Protected Health Information for Reimbursement.
FREE 8+ Sample Hipaa Release Forms in PDF | MS Word

What Will Hipaa Release | Realty Executives Mi : Invoice ...
Free HIPAA Release Form - PDF | 77KB | 2 Page(s)
FREE 11+ HIPAA Release Form Samples in PDF | MS Word
Free Hipaa Forms | amulette

15 Reasons You Should Fall | Realty Executives Mi ...
Medical Release Form Template | charlotte clergy coalition
Hipaa authorization to release medical information form ...
12+ HIPAA Release Form Templates in PDF | DOC | Free ...
HIPAA release forms are an essential part of any effective HIPAA compliance program. This Medical HIPAA Release Form Samples. I, or my authorized representative, request that health information regarding my care and treatment be released as set forth on this form HIPAA Release Form.
